Advanced Building Analytics Leads to Successful Operating Room Optimization
Fifteen years ago, a hospital in Macomb Michigan added a new surgery center wing to their expansive campus and needed building analytics. On the surface, the new addition began as a way to provide quality care with expert surgeries, but deep within the bowels of the hospital, the essential mechanical and control assets serving the new surgery center were suffering from performance issues and band-aid approaches from the very first day of occupancy.
Patient safety and comfort is essential to any high-performing healthcare facility. Since the very opening of the new addition, the surgery center had continual problems with the operating rooms (OR) maintaining proper pressure relationships, which in turn lead to constant issues with temperature and humidity requirements. The ORs were not able to maintain the proper positive pressure relationships required at the design airflow of 25 Air Changes per Hour (ACH), so the Facility Team was forced to increase in the ACH rate in all OR spaces in order to achieve the required positive pressure relationships.
Facility Managers shouldn’t have to run their systems to failure.
This increased Air Changes per Hour (ACH) had a significant cascading impact on the entire system. In order to properly condition the increased airflow required for the modified ACH, the air handling unit (AHU) serving the ORs had to work excessively hard, which included a tremendous increase in its need for more cooling capacity. This demand for more cooling capacity forced the two air-cooled chillers serving the addition to operate well beyond their design capacity, so they were never able to function properly.
For fifteen years they believed the two chillers were the issue within the system as they could never properly meet the cooling requirements of the modified system, so they continued down the path of running the chillers to failure, blowing compressors, replacing equipment, and never being able to truly solve their issues. Eventually, the chillers failed beyond repair and two rental chillers were brought in to keep the system operational. It wasn’t until the addition of building analytics that they were able to discover the root cause of their system troubles and finally put an end to all their headaches.
The demand for more cooling capacity forced the two air-cooled chillers serving the addition to operate well beyond their design capacity, so they were never able to function correctly.
THE PLAN
Three years prior, the Corporate Director of Facilities spearheaded a plan to implement building analytics & fault detection across his entire portfolio of hospitals, 11 sites in total, which proved to be an extremely forward-thinking and beneficial decision for solving the issues at the surgery center. When the root cause continued to go unsolved and the hospital was entering its third year of having two rental chillers on-site, the leadership of the hospital demanded a resolution immediately. In response, the Corporate Director of Facilities decided to leverage the building analytics (fault detection) for the surgical center and have a trusted Engineer do a deep dive into the data to determine a path forward. His Engineer started to analyze the data and worked on-site with the facilities team in order to fully understand the nuances within the facility: the pain points, the trials, the continuous equipment replacement, and the high cost of failure that the facility endured for many years.
The Engineer began by reviewing the original design documents and the most recent test and balance reports to evaluate system functionality compared to current Michigan State guidelines. The Facility Guidelines Institute (FGI) and ASHRAE Standard 170 are the authoritative sources that the State of Michigan adheres to, and those standards state that the minimum required rate should be 20 ACH (Air Change per Hour), while the maximum air change rate (per hospital standards) should be 25 ACH.
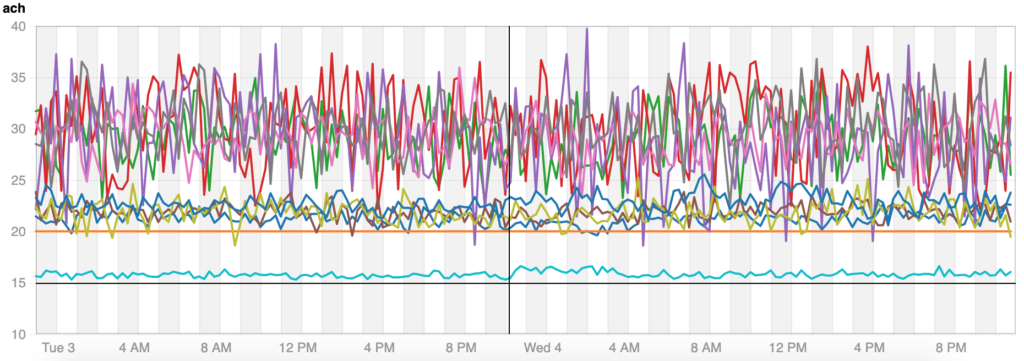
The first obvious problem was that due to the continuous increase in OR airflow over the years in order to maintain positive pressure, all spaces were operating at an air change rate in excess of 35 ACH, with some ORs above 40 ACH. This excessive airflow not only causes pressure relationship nightmares, but it makes maintaining temperature and humidity set-points near impossible. This was the first clue to the Engineer of uncovering the root problem. The chillers were not the problem; it was how they were being operated, they were just trying to respond to system conditions that they simply weren’t designed for. The need for the facility team to excessively increase airflow was due to the poor design of the operating room doors which were never able to seal properly and therefore lead to the constant problems controlling the pressure relationships.
The above data set shows the original flat-blade OR terminal units “hunting” and the Air Changes per Hour they are trying to maintain, all are well above the desired 20 ACH set-point.
It wasn’t until the addition of building analytics that they were able to discover the root cause of their system troubles and finally put an end to all their headaches.
In order to fully understand the extent of the air change rate issues, the Engineer utilized the building analytics already in place. It was revealed in this data that the air pressure relationship issues that the facility was experiencing was being exacerbated by the existing terminal units serving the ORs. Standard flat-blade VAV terminal units were misapplied during the original design; they were not capable and not accurate enough to handle the quick-response needed in the critical application of the ORs. This misapplication led to the VAVs constantly “hunting,” or massive jumps up and down in airflow, in a never-ending attempt to satisfy the temperature and humidity requirements. This type of situation not only causes air pressure relationship issues within the OR, but also causes potential life-safety issues for the patients and staff.
Armed with real-time data and building analytics, a proposal and Return on Investment (ROI) was developed to get the ORs back in compliance with FGI and ASHRAE 170.
The Engineer showed the client this data set which helped visualize the air pressure issues and illustrate the root cause of the problems with the surgery center. Despite earlier assumptions, merely replacing the chillers would not solve the problem. Armed with real-time data and analytics, a proposal and Return on Investment (ROI) was developed to get the ORs back in compliance with FGI and ASHRAE 170 and to achieve substantial energy savings through proper control and optimization.
By reducing the ACH rate from the existing 35+ air changes per hour to 20, an estimated savings of $22,000 per operating room per year could be achieved. In order to accomplish this, the client would need to replace the operating room doors with a modern solution that would seal properly and replace the existing flat-blade VAV terminal units/obsolete controls with proper venturi style terminal units/fast-acting controls that are specifically designed for critical environments. Perhaps more important than the cost of doing this project is the cost of NOT doing the project, which would result in the continuation of $360,000 per year in the cost of rental chillers, an estimated $290,000 per year of lost energy savings, and the immeasurable cost associated with maintaining patient safety.
The cost of NOT doing the project, which would result in the continuation of $360,000 per year in the cost of rental chillers, an estimated $290,000 per year of lost energy savings.
DEPLOYMENT
The client agreed with the plan and began deployment on resolving the longstanding issues. Firstly, the old problematic OR doors were replaced with modern sliding door assemblies per the hospital’s new standards. The new doors would improve patient care, improve infection controls, and solve the air pressure control problems. Secondly, the OR optimization, which included AHU controls upgrades, a modern critical air delivery system utilizing venturi terminal units, and a state-of-the-art critical control system that would accurately maintain proper pressure relationships while controlling to the specific temperature and humidity requirements. Lastly, two new ultra-high efficiency air-cooled chillers would be installed to replace the rental units and to provide the adequate cooling capacity and redundancy needed for the surgery center.
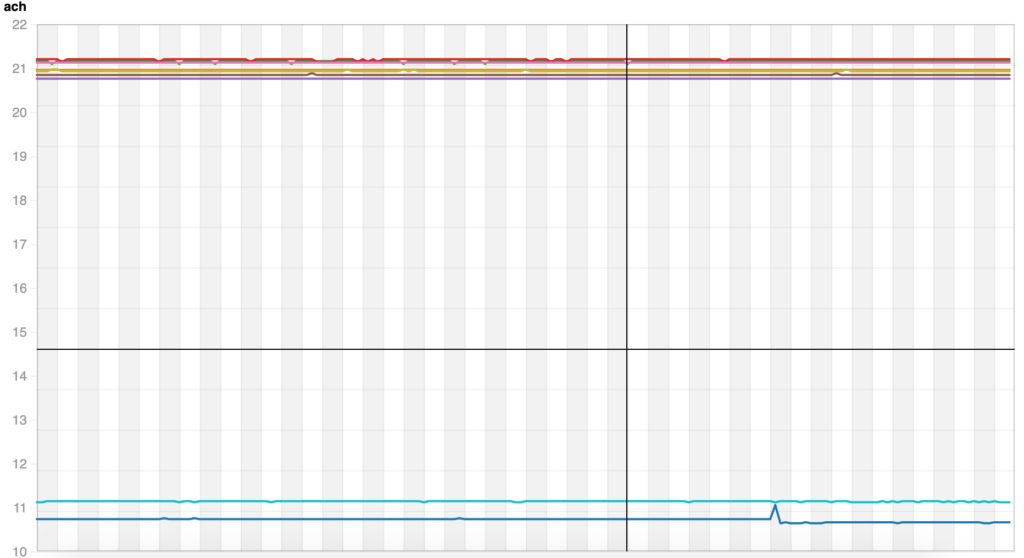
The above data set shows the result of the new critical air delivery system and controls. The ORs are now able to maintain the 21 ACH set-point continuously and the previous “hunting” was eliminated.
Since it was impossible to shut down all the ORs during construction, the Engineer sat down with all groups impacted by the project: site leadership, surgery staff, infectious control, and the facility team to explain the goal of the project and to develop a phasing plan that was in the best interests of all parties. It was also imperative they all understood the impact of the improved control they would have over pressure, temperature, and humidity and how that would benefit not only the efficiency of the surgery center systems, but also the surgery center staff and the safety of their patients. As it was stated early on by the project team, this project was a “no-brainer” to the future success of the surgery center.
LESSONS LEARNED
When recurring problems within a facility become a patient safety issue and a money vacuum, it is valuable to have data available to help diagnose root causes and an experienced Engineer to help determine the proper corrective actions. In this case, it was a long-held belief that the chillers were the main problem, but nothing done to correct the failing chillers solved the issues.
Through the use of the building analytics platform and collaborative site-work with the facility team, the Engineer was able to pin-point the exact source of the problems and develop a proper scope of work and proposal that was seen as a worthwhile investment by the site leadership.
At the time, the hospital did not have a comprehensive plan to properly diagnose and fix the problems at the surgery center, merely keeping the failing equipment operational was the main focus.. However, when these systems finally fail, procedures can’t be performed and patient lives are at risk, not to mention it’s millions of lost revenue at stake. The data not only revealed the source of the existing problems, it also revealed the massive amounts of money lost if the hospital chose not to pursue corrective actions.
OWNER SUCCESS
The visionary Facility Director who implemented the building analytics project across all his campuses enjoyed success and validation from multiple vantage points. From the Facility Team no longer having to keep failing equipment operational, to the relationship between facilities and healthcare staff. And the overall knowledge that the surgery center was no longer a pain-point between the teams. And to the site leadership with empowered data to back up capital planning as well as vital data to prove to the Joint Commission that their critical environments are operating as designed.
The facility team gained insight on a better way to diagnose issues and develop critical projects, through the use of data. This proven template empowered them on how to approach their leadership not only with issues, but also with solutions to those issues. With data pin-pointing problems, they can validate their projects showing energy savings and operational cost savings. This increased confidence in the CFO knowing that their capital plan is dialed in and focused. The transition from band-aid approaches to pro-active solutions through data analysis to drive future capital planning was a big win for the client.